

Issue 14: COVID-19 Knowledge, Practices, and Impacts on Health-Seeking And Provision of Health Services in Rural Tanzania
Global Health Equity Research in Translation brings academic research to broader audiences: decision makers, policy makers, advocacy groups, philanthropists, and journalists. The series draws on transdisciplinary health equity research completed with the support of the Community of Excellence in Global Health Equity at the University at Buffalo, The State University of New York.
I. COVID-19 PANDEMIC AND HEALTH SERVICES


COVID-19 Pandemic
As of late 2020, COVID-19 continues to spread globally. This global health emergency has upended the lives of many across the world with direct and indirect impacts on health. Disruptions to livelihood activities and food systems compounded by overburdening of health systems may have serious impacts on the health and well-being of individuals. Currently, the world is experiencing its largest adolescent population, and adolescence is a key period of development, where investments are thought to have a “triple dividend”, with benefits today, tomorrow and into the next generation (Patton et al. 2014). Adolescents may be acutely vulnerable to overburdened health systems due to pre-existing barriers to their access to sexual and reproductive health services in particular, which the pandemic may exacerbate. During the Ebola epidemic in West Africa, adolescent pregnancy increased, due to a combination of school closures and loss of support networks, as well as overburdened health systems (Sochas et al. 2017). In the Tanzanian context adolescent girls were already vulnerable prior to the pandemic, as 30.5 percent of women were married as a child (before age 18), and 27 percent of adolescent girls aged 15-19 years have given birth (Ministry of Health CD, Gender, Elderly and Children et al. 2017). Policymakers interested in designing programs which can better address the health needs of adolescents and youth (and simultaneously, health of the next generation) in the wake of COVID-19 need more information about how the pandemic is affecting their health and health-seeking behaviors. This brief summarizes mixed method findings around COVID-19 knowledge, attitudes, and practices and how the pandemic has affected health and health-seeking among a sample of adolescents and young peoplei from poor households in the largely rural Iringa and Mbeya Regions of Tanzania.
Executive Summary
We find that information about COVID-19 transmission and prevention measures is reaching this population, but there are gaps in knowledge. Moreover, males reported higher levels of both knowledge and implementation of prevention practices than females. This may be due to more restricted movement and access to technology and resources among females. Participants reported that individuals are relaxing their prevention practices over time. More than one in three health facilities reported decreased ability to provide regular services compared to before March 2020, both due to an increase in COVID-19 caseload and to decreases in staff, funding and supplies. Almost half of facilities reported increases in patients’ difficulties paying for medical services and drugs since the pandemic began, and two-thirds of youth who reported not seeking care when needed cited lack of money as the reason. Taken together, these findings suggest that the COVID-19 pandemic has negatively affected the provision of health services and increased financial barriers to accessing services among patients. Nevertheless, the adolescent population examined here was not as severely affected. Recommendations resulting from this research include continued health communication around the importance of COVID-19 prevention practices, health services strengthening, and programming aimed at economic strengthening.
Methods
This study takes place in Southern Tanzania, in Mbeya located in the South West Highlands and Iringa located in the Southern Highlands zone. Both regions produce cash crops for export, including coffee, tea, and spices. The main sector of employment is agriculture, and the population in these regions face high rates of child stunting, high fertility, and high rates of HIV/AIDS. Data used in this study come from a longitudinal study, which sampled adolescents between the ages of 14 and 19 years (in 2017) living in households participating in the Government’s flagship social protection program, the Productive Social Safety Net (PSSN) (UNICEF Office of Research 2020). Study districts and councils include Mufindi and Mafinga in the Iringa region and Rungwe and Busokelo in the Mbeya region. The study areas (130 villages total) are generally remote, rural villages. For this COVID-19 study, four distinct groups were sampled: adolescents, household heads, community leaders, and health facility staff. The eligibility criteria for adolescents/youth were: being a participant of the existing longitudinal study; and a) being aged 18 years or older; or b) being married and aged 18 years or less.
A total of 760 structured interviews were completed. Among the eligible sample, we purposively selected 46 youth to additionally interview in depth with semi-structured interviews. In addition to data collection among youth, we interviewed a sub-sample of 542 household heads in households where the adolescents live and staff in 83 government-run, primary health care facilities in the study area via mobile phone and asked them four short questions. We also conducted qualitative interviews with 16 randomly selected community leaders. Data collection occurred via mobile phone in September and October 2020. All interviews were conducted in Swahili. Topics covered in the interviews ranged from COVID-19 knowledge prevention; illness and health services utilization; food and water insecurity; time use, including economic activities and chores; mental health; violence; and exploitation. Additional data were collected via SMS with households, youth, and health facilities during the following dates: Round 1: 17 - 30 November; Round 2: 1 - 8 December 2020; Round 3: 15 - 22 December 2020; Round 4: 13 - 20 January 2021. More information on coding and analyses of data can be found in the full report cited at the end of this brief.
Findings
The findings presented here come from quantitative mobile surveys with adolescents/youth (n=760); household heads (n=542); and health facility staff (n=83); as well as qualitative interviews with youth (n=46) and community leaders (n=16). See sample and data collection section for more information.
Limited knowledge of COVID-19 symptoms and sources of information
In the qualitative interviews, most adolescents and youth were able to give some accurate information about the symptoms and transmission of COVID-19. Participants generally knew that symptoms included cough, shortness of breath, and fever, and that the disease could be transmitted through the air. This generally aligned with the survey findings. When asked what were the symptoms of COVID-19, the most common responses were cough (74%), shortness of breath or difficulties breathing (55%), fever (53%), sore throat (25%), tiredness (23%), and loss of taste and/or smell (12%). When aggregated into a scale of symptom knowledge (range 0-10), the average “knowledge” score was only 3.39, however. Males reported higher levels of COVID-19 knowledge than females, and this may reflect their increased freedom of movement in the community and higher rates of paid employment outside the household, where they may be exposed to more sources of information.
Quantitative surveys indicated that the most commonly reported sources of information about COVID-19 included radio (88%), television (58%), community members (33%), friends (32%), and social media (22%). Similarly, qualitative interviews indicated that sources of information about COVID-19 included the media, public health officers, and the government.
Prevention practices aligned with prevailing directives/guidelines
Youth reported receiving the following directives or instructions (in the quantitative survey): avoiding large gatherings (71%), wearing a face mask (70%), washing hands frequently (59%), keeping at least one and a half meters apart from others (36%), and staying home (35%). When asked which measures they actually implemented, youth most commonly reported washing hands with soap and water (82%), wearing a face mask (78%), physical distancing (45%), avoiding touching eyes, nose, and mouth with unwashed hands (36%), and avoiding handshakes (33%). Males reported engaging in prevention measures at higher rates than females, possibly due to their higher levels of COVID-19-related knowledge, or greater overall autonomy.
Qualitative interview participants were also able to correctly identify a number of prevention practices, including mask wearing, social distancing, avoiding crowds, staying home, handwashing, and not shaking hands. Three community respondents and one adolescent mentioned consuming natural remedies as a preventive. For example, one respondent stated, “Most people say garlic… ginger and… lemons help. That is what people were doing, everyone preparing at home and children drinking the mixture as medicine.”
Prevention practices are weakening over time, though. “In fact, they have started to forget being cautious,” said one community participant. Another said, “People no longer remember wearing masks, we go without them to funerals.” Practices like shaking hands and gathering in groups for sports and religious activities were resuming in some areas.
Recent illnesses and symptoms among youth and their families
In the quantitative surveys, 8% reported having been sick in the past month, while 14% reported that a household member had been sick in the same time period. A further 2% of the sample reported a death of a household member in the past month. When asked about the symptoms of their most recent illness (either among the youth or their household member), the most commonly reported symptoms were fever (57%), aches (51%), and headache (37%). It is important to note that there were no confirmed cases of COVID-19 in the households of the participants in the qualitative sample. One adolescent reported having been tested and another that their grandfather had been tested; both of those tests were negative. Eight participants discussed having heard rumors about COVID-19 cases in the broader community, however. Indeed, COVID-19 testing capacity was initially limited to the national laboratory in Dar es Salaam, and so cases from other regions had to be transported to the national laboratory; likely the capacity to transport cases from rural areas was limited. Additionally, unconfirmed cases of fever, aches, and headaches could be from other diseases, including malaria.
Access to health care services
In quantitative surveys, among those who were sick or reported a sick household member (n=148), most sought care at a health center or dispensary (57%), followed by pharmacy (41%) and hospital (24%).ii Despite the pressures COVID-19 placed on the health system, only one of the participants in the qualitative sample said they had difficulty obtaining needed medical care during the pandemic. According to a community leader, people generally “received services as usual.” Several described strict preventive policies that were in place at health facilities: “you are supposed to keep social distance, staying several steps from others in the queue” and “if you are not wearing a mask you are sent home.” The adolescent who reported difficulty getting care said that long lines and crowds at the hospital were barriers to getting routine consultations.
However, participants generally reported wanting to stay away from hospitals and clinics when they could, “because they believed that at the hospital there was danger of infection.” Stigma related to COVID-19 was reported by participants, and this was seen as a reason to avoid hospitals. One community member said that people thought, “If I go [to the hospital] and I am tested, I will be seen by the community like I am different, that I have got an infection.” An adolescent said, “When you go to the hospital, even if it is because of malaria, you would be said to have COVID-19.” In the quantitative survey, among those who reported needed care but did not seek it, 10% reported not seeking care due to a fear of contracting COVID-19, while a majority cited costs as the main reason (67%). Females were more likely than males to not seek care when ill or when needed. This difference may be due to contextual factors such as gender norms, whereby females often need permission from their husbands or household heads to seek health services, or they may have reduced access to financial resources for transport and payment for services, as compared to males.
Barriers to health care utilization
Among the 8% of the quantitative sample who reported not seeking health care when needed in the past month, the biggest reason was lack of money (67%), while 22% reported the distance was too far. These two reasons are often interrelated, as traveling far distances incurs cost of travel and loss of income from taking time off work. Moreover, these findings underscore those summarized elsewhere from this study,iii where participants reported that the strongest impacts in their lives resulting from the COVID-19 pandemic are economic impacts. As a result of the pandemic, the economic insecurity of this vulnerable population has been exacerbated, causing stress, anxiety, food insecurity, and difficulties paying for school-related expenses. One way to improve health care access and reduce financial costs is through coverage by health insurance. Over the course of Government’s social protection program, the PSSN Phase I (2015-2019), PSSN households were encouraged to enroll in Community Health Fund (CHF). Among the sample interviewed over mobile phones (n=542), 31% reported being enrolled in CHF. This is higher than the proportion enrolled nationally, and likely reflects efforts by PSSN implementers to encourage use of the PSSN payments to enroll in CHF. Additionally, Iringa and Mbeya are among the ten regions in Tanzania with the highest rates of CHF enrollment. Among a smaller panel sample of households who responded to the SMS surveys over time (n=95), reported CHF enrolment increased from 28% to 52% between September and November 2020. This may be due to the fact that households received their first PSSN payments of 2020 in September after long delays, and therefore with more available funds, households may have chosen to use these PSSN payments to enroll in CHF. Nevertheless, use of PSSN payments for enrollment in CHF is not a sustainable solution for healthcare coverage among poor households.
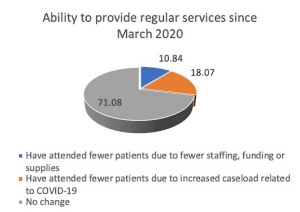
Healthcare utilization is also influenced by available services during the pandemic. Turning to the interviews with health facility staff, responses were varied about whether there were changes in caseloads before and after March 2020. Thirty-seven percent of facilities reported a decrease in caseload, while 29% reported an increase, and 38% reported no change. Most (71%) reported no change in their ability to provide regular services (including well-baby check-ups, vaccinations, maternal health, family planning, etc.) compared to before March 2020. However, 18% did report attending fewer patients for regular services due to increased caseload related to COVID-19, while another 11% reported attending fewer patients for regular services due to reductions in staffing, funding, or supplies (Figure 1). In addition, 46% of health facilities reported noticing increases in patients’ difficulties in paying for medical services and drugs since March 2020.
Figure 1: Health Facilities Mobile Survey (n=83)

II. TAKEAWAYS
Information about COVID-19 has reached youth (as reported by a mobile data survey). There was accurate knowledge of some symptoms of COVID-19; however only three symptoms were recognized by more than half the sample. Common sources of information included radio, television, friends and neighbors, and social media. Respondents did report implementing prevention measures, including washing hands, wearing a mask and social distancing. Recent relaxing of social distancing measures may be a result of messaging by Government, as President Magufuli declared the Tanzania coronavirus outbreak “absolutely finished” in June 2020 (Dahir 2020). Very few respondents reported not seeking care when needed in the past month. Among those who did report not seeking care when needed, lack of money was the most common reason. Females, on average, had lower levels of reported knowledge and reported implementing prevention measures at lower rates than males. Females were also more likely to not seek care when needed. Enrollment in CHF, which can help alleviate the financial burden of seeking care, was reported by only one third of households in the sample, indicating the need to expand health insurance coverage among this population. Despite these gaps in coverage, the rates are still higher than those nationally and likely reflect integration efforts by PSSN implementers, who encouraged participants in this anti-poverty program to use cash transfers from the program to enroll in the CHF. Nevertheless, use of PSSN payments for enrollment in CHF is not a sustainable solution for healthcare coverage among poor households. Despite the sample of youth generally not reporting difficulties accessing care when needed, almost half of facilities reported noticing increased difficulties’ in patient’s ability to pay for services and medicines, and staff at almost one-third of health facilities report a reduction in the ability to provide general services, compared to the period before March 2020. Reasons indicated for this reduction in regular services related to increased COVID-19 caseload and having fewer resources, staff, or supplies. This suggests that COVID-19 has had an adverse impact on the delivery of health care services, and this may have medium- and longer-term effects on unintended pregnancy, nutrition, and lower vaccination rates, among others.
This study has provided real-time information on how COVID-19 is affecting health services utilization and capacity to deliver health services. The most salient impacts reported in the study overall were those related to increased economic insecurity, which may have future negative implications for health. Limitations of the study include the nature of the data collection over the phone and the fact that we leveraged an existing sample, which was comprised of adolescents and youth, who tend to be healthier, on average, than other segments of the population. Thus, in terms of direct health impacts of COVID-19 infection, adolescents and young adults might be among the least vulnerable. Another recent report also noted that COVID-19 had yet to have severe health or economic consequences in Tanzania, but that women in the country were among the most vulnerable globally, should effects materialize.iv Nevertheless, social distancing, school closures, and reduced capacity at among the poorest 10% of the population (based on PSSN targeting) and live in remote, rural villages. Thus, their health and ability to access services may be adversely affected through more economic channels.
Recommendations for future programming include:
- Continued health communication: Qualitative findings suggested that people in the targeted communities are beginning to relax their COVID-19 prevention practices, including social distancing and mask wearing. Therefore, we recommend continued focus on these practices in all ongoing projects by Government and development partners.
- Improved informational channels: While most participants had some degree of knowledge about COVID-19 symptoms, there were gaps in understanding. This suggests that more work needs to be done to understand the information that Tanzanians are receiving about COVID-19 and how this information delivery can be improved.
- Health services strengthening: Support could be given to health facilities in terms of reinforced staffing and financial support to ensure smooth delivery of services, including those related to COVID-19 but also regular services during this time of increased demand.
- Economic strengthening: Reported barriers to seeking care often were demand-side barriers related to poverty. In the larger study, economic impacts were the most salient related to COVID-19, as households faced reduced income, increasing prices, and difficulties accessing some basic goods. Various economic strengthening initiatives can mitigate these adverse impacts of the global pandemic and future shocks on health. Initiatives may include expanding social protection coverage and ensuring that payments are regular, as well as other initiative such as scaling up agricultural extension programming to promote resiliency and increased productivity of crop production and livestock keeping.
- Expand coverage of social health protection including enrollment in the Community Health Fund: Currently, enrollees, including those from poor households in the PSSN, have to pay annual premiums for coverage. Initiatives could be designed by the government and development partners, whereby premiums for those households below the extreme poverty line are covered by alternative sources of funding, instead of by households.
REFERENCES
Dahir A. 2020. Tanzania’s President Says Country Is Virus Free. Others Warn of Disaster. The New York Times.
Ministry of Health CD, Gender, Elderly and Children, Ministry of Health, National Bureau of Statistics, [Zanzibar] OoCGS. 2016. Tanzania Demographic and Health Survey and Malaria Indicator Survey 2015-2016. MoHCDGEC, MOH, National Bureau of Statistics and ICF.
Patton, G.C., Ross, D.A., Santelli, J.S., Sawyer, S.M., Viner, R.M., & S. Kleinert. 2014. Next steps for adolescent health: a Lancet Commission. The Lancet 383(9915): 385-386.
Sochas, L., Channon, A.A., & S. Nam. 2017. Counting indirect crisis-related deaths in the context of a low-resilience health system: the case of maternal and neonatal health during the Ebola epidemic in Sierra Leone. Health Policy and Planning 32(suppl_3): iii32-iii39.
UNICEF Office of Research - Innocenti. 2020. Tanzania Cash Plus Evaluation Team. A Cash Plus Model for Safe Transitions to a Healthy and Productive Adulthood. Round 3 Report.
ACKNOWLEDGEMENTS
Funding for this mobile study on COVID-19 impacts has generously been provided by UNICEF Tanzania and Deutsche Gesellschaft für Internationale Zusammenarbeit GIZ GmbH under the umbrella of the P4H Health Financing Network. This study leveraged a cohort from an on-going study entitled “A Cash Plus Model for Safe Transitions to a Healthy and Productive Adulthood” (2017-2019), and the latter was funded by Oak Foundation (#OCAY-16-73), the UK’s Department of International Development (DFID 203529-102), the Swedish Development Cooperation Agency (Sida G41102), and Irish Aid.
AUTHORS
Tia Palermo, Stephanie Zuilkowski, Sarah Quiñones, Graca Marwerwe, Hassan Kihanzah, Leah Prencipe, and Lusajo Kajula
RECOMMENDED CITATION
Palermo, Tia, Zuilkowski, Stephanie, Quiñones, Sarah, Marwerwe, Graca, Kihanzah, Hassan, Prencipe, Leah, and Kajula, Lusajo. COVID-19 Knowledge, Practices, and Impacts on Health-Seeking and Provision of Health Services in Rural Tanzania - Research Brief. Global Health Equity Research in Translation. Eds. Emmanuel Frimpong Boamah, Katarzyna Kordas, and Samina Raja. Community of Excellence in Global Health Equity, March 2021.
SOURCE TEXTS
Tia Palermo, Stephanie Zuilkowski, Sarah Quiñones, Graca Marwerwe, Hassan Kihanzah, Leah Prencipe, and Lusajo Kajula, on Behalf of the Tanzania Adolescent Cash Plus Evaluation Team. (2020). “Real-time monitoring of COVID-19 impact among adolescents and young people, their families, and communities in Southern Highlands regions in Tanzania.” UNICEF Tanzania and University at Buffalo: Dar es Salaam and Buffalo.
SERIES EDITORS
Dr. Emmanuel Frimpong Boamah, Dr. Katarzyna Kordas, and Dr. Samina Raja
DESIGN
Nicole Little
PRODUCTION
Alex Judelsohn
FOOTNOTE(S)
[i]The National Policy of Youth Development (2007) in Tanzania defines youth as individuals aged 15-35 years.
[ii] Totals exceed 100% because respondents could report more than one source for seeking care.
[iii] Tia Palermo, Stephanie Zuilkowski, Sarah Quiñones, Graca Marwerwe, Hassan Kihanzah, Leah Prencipe, and Lusajo Kajula, on Behalf of the Tanzania Adolescent Cash Plus Evaluation Team. (2020). “Real-time monitoring of COVID-19 impact among adolescents and young people, their families, and communities in Southern Highlands regions in Tanzania.” UNICEF Tanzania and University at Buffalo: Dar es Salaam and Buffalo.
[iv] Buvinic, M., et al. (2020). Understanding Women’s and Girls’ Vulnerabilities to the COVID-19 Pandemic: A Gender Analysis and Data Dashboard of Low- and Lower-Middle Income Countries. Washington, DC, Data2x and Open Data Watch.